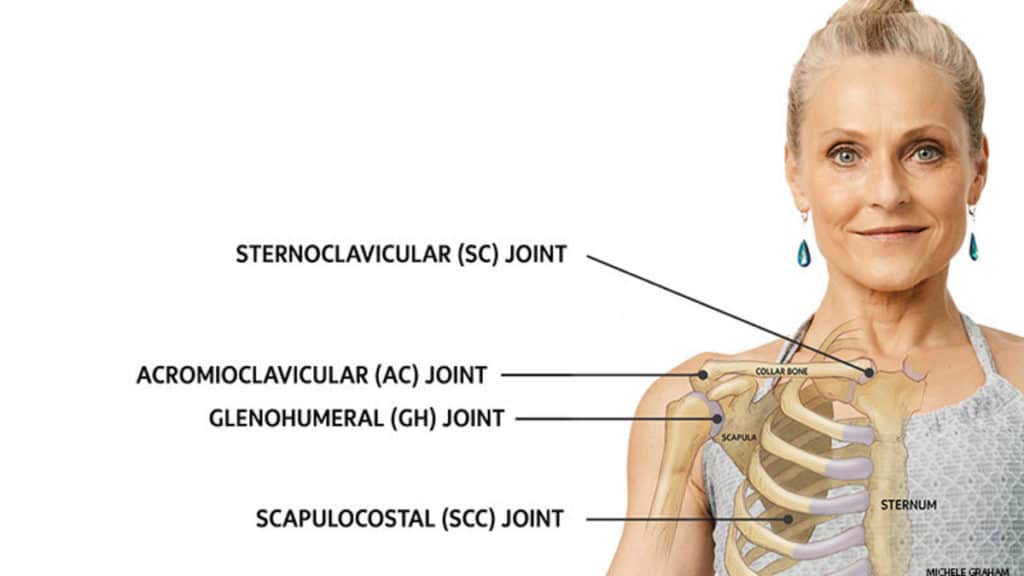
Dislocation of Sternoclavicular Joint and Acromioclavicular Joint Injury
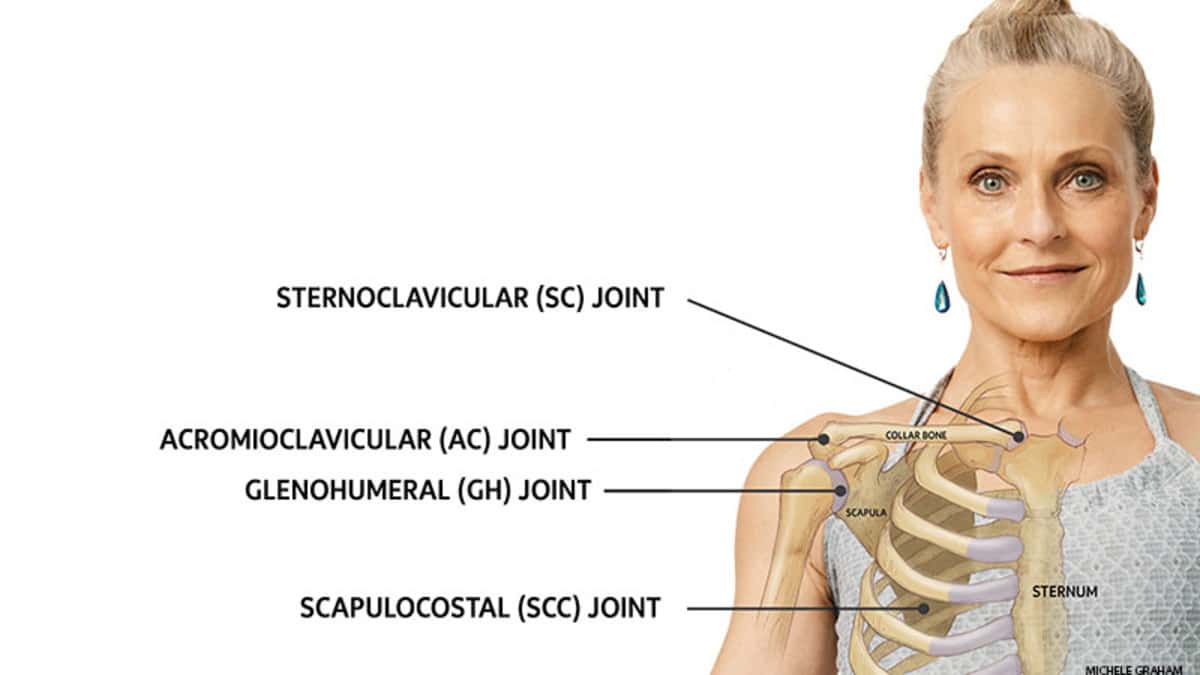
Dislocation of sternoclavicular joint is not a common condition. The joint is firmly supported by the capsule and ligaments around the joint and by the strong costoclavicular ligament from below. This can bear the burden of severe sprain without being displaced. Mechanism of Injury: The lesion is produced mainly due to indirect violence, but direct injury can lead to the same result.
Indirect Force: When one falls on an outstretched hand the force is directed along the upper limb to the shoulder- joint and transmitted to the sternoclavicular joint. The force impinges against the sternum with displacement of the clavicle.
Direct Injury: Direct injury over the medial end of clavicle can displace it posteriorly.
Types of Dislocation: In case of complete dislocation there is rupture of the costoclavicular ligament. The displacement may be anterior, superior or posterior.
DIAGNOSIS
It is easy to make the diagnosis by clinical examination. Localized lump along with tenderness can be detected over the sternoclavicular joint. Shoulder- joint movement produces pain. In severe posterior dislocation, the sternal end of clavicle can press over the trachea producing acute respiratory distress.
TREATMENT
Reduction by manipulation can sometimes be done easily when performed at an early stage. The anatomical nature of the joint is such that it is difficult to maintain the correct position even after successful reduction. Failure to reduce the dislocation properly will lead either to unreduced dislocation, or subluxation of the joint. Person with unreduced dislocation can perform normal activity without any disability. The presence of a lump reduced by unsuccessful reduction will not produce a good cosmetic result.
Technique of Reduction: Most cases cab be dealt with without any anaesthesia. This can also be done by infiltrating local anaesthetic solution over the site of dislocation or by giving general anaesthesia. Reduction can be performed in one of three ways.
- The patient site on a stool and the surgeon pulls the shoulder joints of the patient backwards and supports the back with the flexed knee.
- Patient lies supine on the table. A sand bag is placed under the intercapsular area to elevate the shoulder- joints. The surgeon then presses both the shoulder- joints posteriorly.
- Patient’s upper limb of the affected part is pulled in an abducted position. The assistant maintains the countertraction from the opposite side.
Correction of Anterior or Posterior Dislocation
In anterior dislocation: The sternal end of the clavicle is pressed posteriorly while the traction on the limb is maintained.
In posterior dislocation: While the lateral traction on the clavicle is maintained by the assistant, this is elevated by pulling forward with the aid of the surgeon’s fingers.
Maintenance of Reduction: Reduction is maintained by applying figure of eight bandage as done in the case of fracture clavicle.
Plaster Immobilization: In selected cases plaster immobilization in the form of figure of eight bandage may prove effective.
Management: This is done on the same principle as in the case of fracture clavicle. Immobilization is maintained for a period of six weeks.
Operative Procedure: Surgery is done only on rare occasions. Besides cosmetic reasons, operation can be undertaken due to pain following unreduced dislocation. Open reduction and fixation of clavicle to sternum with fascial graft or metallic wire are done. Urgent open reduction is required in posterior dislocation when there is compression on the trachea and vessels are present. The medical implants like metallic wire for the surgery are manufactured by various orthopedic implants importers.
ACROMIOCLAVICULAR JOINT INJURY
The clavicle maintains its lateral attachment by the capsule surrounding the acromioclavicular joint and by the firm fixation of coracoclavicular ligament from below.
Mechanism of Injury: Most of the traumatic lesions are produced by direct injury as seen usually during athletic activities.
Types of Injury: Three types of injury can affect the joints. They are:
- Sprain.
- Subluxation.
- Dislocation.
SPRAIN OF THE ACROMIOCLAVICULAR JOINT
The ligaments of the acromioclavicular joint remain intact, only a few of the fibres are stretched or torn. There is no damage to the ligaments between the coracoid process and the clavicle.
DIAGNOSIS
Pain, swelling and tenderness develop over the joint. The level of the clavicle is maintained at the normal position. No upward or downward mobility of the clavicle can be detected by applying pressure on the bone.
X- Ray: Radiology does not reveal any abnormality. The normal shoulder joint can also be x-rayed for comparison.
TREATMENT
Management is simple and is directed towards the immobilization of the upper limb by cuff and collar sling or triangular bandage. This is maintained for a period of 8-10 days. Active exercises of the shoulder is advocated at the end of immobilization.
SUBLUXATION OF THE ACROMIOCLAVICULAR JOINT
In subluxation there is partial or complete tear of the acromioclavicular joint but the conoid and trapezoid part of the ligament remains unaffected.
DIAGNOSIS
The patient usually holds his affected limb with the opposite one. There are pain and swelling over the joint. There is elevation of the outer end of clavicle and mobility can be detected by applying pressure with the examination finger.
X-ray: Radiological investigation cannot replace the clinical diagnosis. The normal acromioclavicular joint may also be x-rayed along the injured one for comparison. The joint space is increased and outer end of clavicle is found to be at a higher level.
TREATMENT
The whole procedure can be performed without any anaesthesia. Felt pad or cotton wool is placed over the joint. The clavicle is pressed with the finger to depress it into its normal position. Two- inch wide elastoplast is then strapped from above the joint surface of the arm, elbow joint and posterior surface of the ram. Cuff and collar sling is applied. The weight of the limb and strapping keep the clavicle in a depressed position. Immobilization is maintained for 3 weeks. Strapping should be replaced by a fresh one when it becomes loose. Progressive exercise is instituted after the period of immobilization. Failure to reduce the subluxation may not produce any disability and no further treatment is required.
DISLOCATION OF THE ACREMIOCLAVICULAR JOINT
In case of acromioclavicular dislocation, there is complete rupture of the ligamentous attachment of clavicle with coracoid and acromion processes. The tension of the trapezius and sternomastoid muscles lifts the clavicle above and behind the acromion process.
DIAGNOSIS
The unusual swelling produced by the displaced clavicle is characteristic. The whole length of the clavicle is directed more posteriorly in comparison to the normal one.
X-ray: There is wide separation of the joint-space.
TREATMENT
Reduction: In most cases reduction by closed method is all that is necessary. Surgery is needed only on rare occasions and when surgery is needed, surgeons need various orthopedic implants and instruments to perform it.
Closed Reduction: Firm encircling strapping is done in the same way as in the case of subluxation of the joint. Immobilization is maintained for a period of 4-5 weeks. Even in cases of unreduced dislocation the disability may not be of much concern.
Operative Reduction: Three different types of operation may be performed.
- Kirschner’s wire fixation between the clavicle and acromion process.
- Reconstruction of conoid and trapezoid ligaments by fascia lata.
- Excision of the lateral third of clavicle when pain is produced due to unreduced dislocation.